
The Starkness of Health Inequities between Blacks and Whites
The Starkness of Health Inequities between Blacks and Whites
Myth 3, Part 2

(The feedback I received on my last post: it was really interesting and very, very long. Length in writing is my Achilles heel. The post was my longest by double. I’m working to rein myself in! Let me know how I do this time.)
When tennis superstar Serena Williams gave birth to her daughter Alexa in September 2017, she, like too many Black women, had difficulty at the last stage of her pregnancy and giving birth. Her daughter’s heart rate increased dramatically, leading to an emergency C-section.
Fortunately, Williams’ C-section birth was successful, but almost immediately after, she experienced even greater difficulty: a pulmonary embolism within 24 hours after giving birth; her coughing due to the embolism led to tearing open the stitching from the C-section; when doctors returned to her surgery, they found significant swelling of clotted blood in her abdomen; finally, a procedure to prevent further clotting that might migrate to her lungs. However, Serena had to convince hospital staff to give her a CT scan when she began to lose feeling in her legs and experience a significant increase in pain. Only after several conversations pressing staff for immediate follow-up diagnosis of her condition because she knew she was at risk of blood clots.

Williams was fortunate because she had access to excellent care. That is not always the case for African American women.
Health inequities between Whites and Blacks start before, at, and in the days and months after birth.
“Black women are 50% more likely to have a premature baby than white women (C.D.C.). Preterm birth, or delivery before 37 weeks of pregnancy, can result in higher rates of death and disability.”[1]
Black infants are two times more likely to die by age one than White infants, a percentage gap larger than what was true during slavery.[2] [3] You may know that premature births can increase the risk that when those babies become adults, they are more likely to suffer chronic diseases than the general population.[4]
Even after a woman has passed the high-risk stages pre-natally and in the days and weeks after birth, the risks are not over.
In formerly redlined areas, Black women more often suffer significant mental health challenges after giving birth than women living elsewhere. These health challenges tend not to be well addressed or treated. The challenges include “severe maternal depression, chronic stress, substance use disorder, and pregnancy-related hypertension. This, coupled with the fact that Black women are three times more likely to die due to pregnancy-related complications than white women (according to the U.S. Centers for Disease Control), is causing some expecting mothers to be ‘terrified of giving birth.’ “[5]
Thus, once again, we see that where people live in America matters. The challenges African Americans face transcend beyond pre-natal-, post-natal, and maternity care. We see profound health inequities between Blacks and Whites across the board.
If you read my last post, you would probably speculate that exposure to nearly every type of pollution and toxin I recounted would lead to poorer health outcomes for Blacks. Your speculation would be correct.
Cruelty Toward Blacks: Important Dimension of our U.S. Medical History
What preceded these exposures to toxic pollution for the past century in some cases and ran parallel in others were a series of troubling, often horrific medical episodes that, to this day, make many African Americans rightly suspicious of the U.S. health and medical sector:
Cruel experimentation during our nation’s lengthy period of enslavement
Involuntary sterilization for the better part of the 20th century (approximately 1907 to the early 1970s). Although Black women were a primary target, targets also included Native American women and those of Puerto Rican descent
Profoundly unethical behavior of an African American woman’s cancer cells that many pharmaceutical and private research companies profited from
Changing medical education standards to intentionally preclude the training of Black doctors who were viewed as not capable of becoming medical doctors. The new standards caused the closing of five of the seven Black medical institutions at that time, meaning the training of Black doctors slowed to a trickle for decades. One study estimated it prevented the additional training of up to 30,000 Black doctors for several decades in the U.S.
The infamous Tuskegee Syphilis Study, in which White researchers intentionally allowed 400 Black farmers who were a part of the study to live without access to penicillin for the last 30 years of the study.
This list could go on much longer, but these depressing episodes will suffice to make the point. I will write more about trust and faith in medical systems in Part 3.
In modern times, many factors contribute to one’s health or lack thereof.
Social Determinants of Health
In fact, a relatively small yet essential part of health depends on high-quality healthcare. Experts say it only accounts for about 10–20 percent of the health outcomes of individuals. Ideally, such care is not just high quality but also affordable.
But what about the other 80–90 percent? That much higher percentage involves what scientists call the social determinants of health. That is, the health choices that individuals often face are not always entirely under their control. Socioeconomic circumstances play a much more significant role in an individual’s health.[6]
These determinants include
the economic stability of the individuals and the communities in which they live;
the elements of the built environment these individuals encounter there, like proximity to pollution and other environmental hazards, as well as their access to green/open/recreational spaces;
the access they have to quality healthcare, education, and food;
the level of social and community stress residents regularly experience, including experiences of high rates of poverty and exposure to high rates of crime, for example.[7]
Differences in Life Expectancy
It should be no surprise, then, that social determinants of health impact life expectancy.
Life expectancy for African Americans improved significantly during the twentieth century and continued into the twenty-first. In 1900, the difference in life expectancy between Black people and White people stood at fifteen years because of a very high infant mortality rate for Black children. Equally important, because of pervasive, lawful discrimination and segregation, Blacks had abysmal access to quality care. The differences in life expectancy began to narrow during the 1970s as Black people gained access to Medicare and Medicaid if they didn’t have private insurance.
However, Blacks’ progress stalled in bridging the life expectancy gap from the early 1980s to the mid-1990s primarily because of much higher homicide and AIDS infection rates than Whites. After 1995, the gap in life expectancy between Blacks and Whites narrowed considerably, again, due to lower rates of infant mortality, homicide, and AIDS infection rates and better treatment for cardiovascular diseases and cancer. By 2014, the gap stood at just less than four years.[8] [9]
So, there is very positive news, overall, on life expectancy. However, variations within and across geographies matter for Blacks and Whites.
Studies show that African Americans die earlier than White Americans across the board on critical health issues. They are more than 40 percent likely, overall, to die between the ages of 18 and 64. Specifically, Black people are far more likely to die within three age bands—18 to 34, 35 to 49, 50 to 64—for high blood pressure, diabetes, and stroke.[10] These facts are not only disheartening; they’re damning.
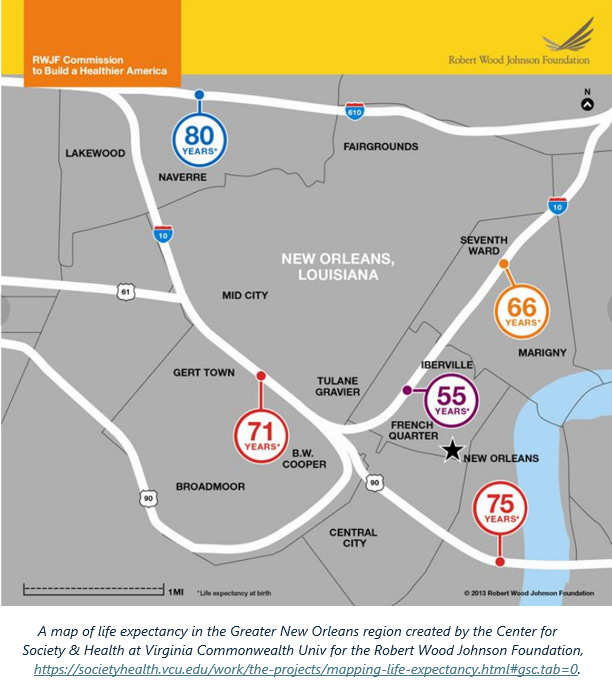
In their initiative “Mapping Life Expectancy,” Virginia Commonwealth researchers showed that where you live “can have more to do with how long you live than your D.N.A., medical history, insurance status, or experience with the health care system. When it comes to good health, our ZIP code can be more important than our genetic code.”[11] They found that majority–African American neighborhoods are more likely to have fewer hospitals and worse access to providers that offer lower-quality care (e.g., community health centers, emergency rooms, outpatient care) than majority-White neighborhoods. The neighborhoods where Blacks live, in general, also tend to have healthcare shortages in primary care, dental health, and mental health.[12]
Thus, what has become eminently clear is that Blacks are impacted negatively by more social determinants—e.g., food insecurity, poorer access to healthcare, higher rates of unemployment and underemployment, etc.—than Whites.[13]
I’ll continue this exploration later in the week in Part 3.
NOTE: the map you see above of the Greater New Orleans region is one of more than two dozen large metro regions that can be found at this link on the Center for Society and Health website.
FOOTNOTES
[1] Dominique Stewart, “Support Black Motherhood,” Anti-Racism Daily, November 30, 2021.
[2] Rashawn Ray, et al., “Examining and Addressing COVID-19 Racial Disparities in Detroit,” The Brookings Institution, 2021.
[3] Steven Woolf, et al., “How conditions for wellness vary across the metropolitan Washington region,” Virginia Commonwealth Center on Society and Health, October 2018, p. 9.
[4] Stewart, November 30, 2021
[5] Stewart, November 30, 2021.
[6] Steven Woolf, et al., “How conditions for wellness vary across the metropolitan Washington region,” Virginia Commonwealth Center on Society and Health, October 2018, p. 6, https://www.mwcog.org/documents/2020/10/26/uneven-opportunities-how-conditions-for-wellness-vary-across-the-metropolitan-washington-region-health-health-data/.
[7] Samantha Artiga, Kendal Orgera, and Olivia Pham, “Disparities in Health and Health Care: Five Key Questions and Answers,” Kaiser Family Foundation, March 4, 2020, https://www.kff.org/disparities-policy/issue-brief/disparities-in-health-and-health-care-five-key-questions-and-answers/.
[8] Sam Harper, John Lynch, Scott Burris, and George Davey Smith, “Trends in the black-white life expectancy gap in the United States, 1983–2003,” Journal of the American Medical Association, March 21, 2007, 297:11, pp. 1224–32.
[9] Woolf, et al., pp. 7–9.
[10] “African American Health Disparities,” DiversityNursing.com, September 15, 2017, https://diversitynursing.com/african-american-health-disparities/.
[11] Woolf, et al.
[12] Jamila Taylor, “Racism, Inequality, and Health Care for African Americans,” The Century Foundation, December 19, 2019, pp. 5–6, https://tcf.org/content/report/racism-inequality-health-care-african-americans/.
[13] Andrew Yawn, “Study finds that eight factors put Black adults at greater risk of early death,” Tulane University School of Public Health and Tropical Medicine, June 2023, https://sph.tulane.edu/study-finds-eight-factors-put-black-adults-greater-risk-early-death.